Cost-Effectiveness of Mobile Stroke Unit Care in Norway
| dc.contributor.author | Lund, Ulrikke Højslev | |
| dc.contributor.author | Stoinska-Schneider, Anna Karina | |
| dc.contributor.author | Larsen, Karianne | |
| dc.contributor.author | Bache, Kristi Cecilie Grønvold | |
| dc.contributor.author | Robberstad, Bjarne | |
| dc.date.accessioned | 2022-11-16T10:01:57Z | |
| dc.date.available | 2022-11-16T10:01:57Z | |
| dc.date.created | 2022-10-21T11:08:28Z | |
| dc.date.issued | 2022 | |
| dc.identifier.issn | 0039-2499 | |
| dc.identifier.uri | https://hdl.handle.net/11250/3032094 | |
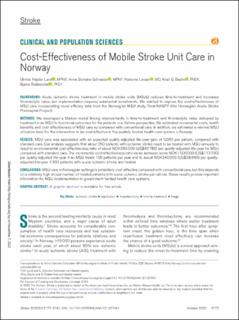
| dc.description.abstract | Background: Acute ischemic stroke treatment in mobile stroke units (MSUs) reduces time-to-treatment and increases thrombolytic rates, but implementation requires substantial investments. We wanted to explore the cost-effectiveness of MSU care incorporating novel efficacy data from the Norwegian MSU study, Treat-NASPP (the Norwegian Acute Stroke Prehospital Project). Methods: We developed a Markov model linking improvements in time-to-treatment and thrombolytic rates delivered by treatment in an MSU to functional outcomes for the patients in a lifetime perspective. We estimated incremental costs, health benefits, and cost-effectiveness of MSU care as compared with conventional care. In addition, we estimated a minimal MSU utilization level for the intervention to be cost-effective in the publicly funded health care system in Norway. Results: MSU care was associated with an expected quality-adjusted life-year-gain of 0.065 per patient, compared with standard care. Our analysis suggests that about 260 patients with ischemic stroke need to be treated with MSU annually to result in an incremental cost-effectiveness ratio of about NOK385 000 (USD 43 780) per quality-adjusted life-year for MSU compared with standard care. The incremental cost-effectiveness ratio varies between some NOK1 000 000 (USD 113 700) per quality-adjusted life-year if an MSU treats 100 patients per year and to about NOK340 000 (USD 38 660) per quality-adjusted life-year if 300 patients with acute ischemic stroke are treated. Conclusions: MSU care in Norwegian settings is potentially cost-effective compared with conventional care, but this depends on a relatively high annual number of treated patients with acute ischemic stroke per vehicle. These results provide important information for MSU implementation in government-funded health care systems. | en_US |
| dc.language.iso | eng | en_US |
| dc.publisher | Wolters Kluwer | en_US |
| dc.rights | Attribution-NonCommercial-NoDerivatives 4.0 Internasjonal | * |
| dc.rights.uri | http://creativecommons.org/licenses/by-nc-nd/4.0/deed.no | * |
| dc.title | Cost-Effectiveness of Mobile Stroke Unit Care in Norway | en_US |
| dc.type | Journal article | en_US |
| dc.type | Peer reviewed | en_US |
| dc.description.version | publishedVersion | en_US |
| dc.rights.holder | Copyright 2022 the authors | en_US |
| cristin.ispublished | true | |
| cristin.fulltext | original | |
| cristin.qualitycode | 2 | |
| dc.identifier.doi | 10.1161/STROKEAHA.121.037491 | |
| dc.identifier.cristin | 2063626 | |
| dc.source.journal | Stroke | en_US |
| dc.source.pagenumber | 3173-3181 | en_US |
| dc.identifier.citation | Stroke. 2022, 53 (10), 3173-3181. | en_US |
| dc.source.volume | 53 | en_US |
| dc.source.issue | 10 | en_US |
Files in this item
This item appears in the following Collection(s)

Except where otherwise noted, this item's license is described as Attribution-NonCommercial-NoDerivatives 4.0 Internasjonal