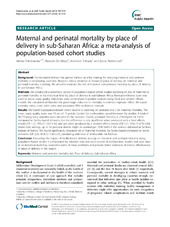
Maternal and perinatal mortality by place of delivery in sub-Saharan Africa: a meta-analysis of population-based cohort studies
| dc.contributor.author | Chinkhumba, Jobiba | en_US |
| dc.contributor.author | De Allegri, Manuela | en_US |
| dc.contributor.author | Muula, Adamson S. | en_US |
| dc.contributor.author | Robberstad, Bjarne | en_US |
| dc.date.accessioned | 2014-10-09T12:21:04Z | |
| dc.date.available | 2014-10-09T12:21:04Z | |
| dc.date.issued | 2014-09-28 | eng |
| dc.identifier.issn | 1471-2458 | |
| dc.identifier.uri | https://hdl.handle.net/1956/8624 | |
| dc.description.abstract | Background: Facility-based delivery has gained traction as a key strategy for reducing maternal and perinatal mortality in developing countries. However, robust evidence of impact of place of delivery on maternal and perinatal mortality is lacking. We aimed to estimate the risk of maternal and perinatal mortality by place of delivery in sub-Saharan Africa. Methods: We conducted a systematic review of population-based cohort studies reporting on risk of maternal or perinatal mortality at the individual level by place of delivery in sub-Saharan Africa. Newcastle-Ottawa Scale was used to assess study quality. Outcomes were summarized in pooled analyses using fixed and random effects models. We calculated attributable risk percentage reduction in mortality to estimate exposure effect. We report mortality ratios, crude odds ratios and associated 95% confidence intervals. Results: We found 9 population-based cohort studies: 6 reporting on perinatal and 3 on maternal mortality. The mean study quality score was 10 out of 15 points. Control for confounders varied between the studies. A total of 36,772 pregnancy episodes were included in the analyses. Overall, perinatal mortality is 21% higher for home compared to facility-based deliveries, but the difference is only significant when produced with a fixed effects model (OR 1.21, 95% CI: 1.02-1.46) and not when produced by a random effects model (OR 1.21, 95% CI: 0.79-1.84). Under best settings, up to 14 perinatal deaths might be averted per 1000 births if the women delivered at facilities instead of homes. We found significantly increased risk of maternal mortality for facility-based compared to home deliveries (OR 2.29, 95% CI: 1.58-3.31), precluding estimates of attributable risk fraction. Conclusion: Evaluating the impact of facility-based delivery strategy on maternal and perinatal mortality using population-based studies is complicated by selection bias and poor control of confounders. Studies that pool data at an individual level may overcome some of these problems and provide better estimates of relative effectiveness of place of delivery in the region. | en_US |
| dc.language.iso | eng | eng |
| dc.publisher | BioMed Central | eng |
| dc.relation.ispartof | <a href="http://hdl.handle.net/1956/17491" target="blank"> Economic analysis of Resultsbased financing in Malawi. Strengthening the evidence base for alternative maternal and perinatal Healthcare funding</a> | |
| dc.rights | Attribution CC BY | eng |
| dc.rights.uri | http://creativecommons.org/licenses/by/2.0 | eng |
| dc.subject | Maternal and perinatal mortality risk | eng |
| dc.subject | Place of delivery | eng |
| dc.subject | Sub-Saharan Africa | eng |
| dc.title | Maternal and perinatal mortality by place of delivery in sub-Saharan Africa: a meta-analysis of population-based cohort studies | en_US |
| dc.type | Peer reviewed | |
| dc.type | Journal article | |
| dc.date.updated | 2014-10-08T19:04:07Z | |
| dc.description.version | publishedVersion | en_US |
| dc.rights.holder | Copyright 2014 Chinkhumba et al.; licensee BioMed Central Ltd. | |
| dc.rights.holder | Jobiba Chinkhumba et al.; licensee BioMed Central Ltd. | |
| dc.source.articlenumber | 1014 | |
| dc.identifier.doi | https://doi.org/10.1186/1471-2458-14-1014 | |
| dc.identifier.cristin | 1215235 | |
| dc.source.journal | BMC Public Health | |
| dc.source.40 | 14 |
Tilhørende fil(er)
Denne innførselen finnes i følgende samling(er)

Med mindre annet er angitt, så er denne innførselen lisensiert som Attribution CC BY