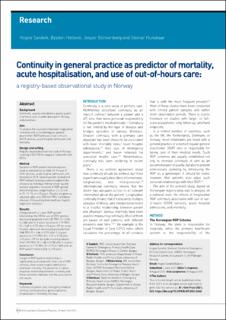
Continuity in general practice as predictor of mortality, acute hospitalisation, and use of out-of-hours care: a registry-based observational study in Norway
| dc.contributor.author | Sandvik, Hogne | |
| dc.contributor.author | Hetlevik, Øystein | |
| dc.contributor.author | Blinkenberg, Jesper | |
| dc.contributor.author | Hunskaar, Steinar | |
| dc.date.accessioned | 2022-02-16T13:41:18Z | |
| dc.date.available | 2022-02-16T13:41:18Z | |
| dc.date.created | 2021-10-04T17:53:44Z | |
| dc.date.issued | 2022 | |
| dc.identifier.issn | 0960-1643 | |
| dc.identifier.uri | https://hdl.handle.net/11250/2979429 | |
| dc.description.abstract | Background Continuity, usually considered a quality aspect of primary care, is under pressure in Norway, and elsewhere. Aim To analyse the association between longitudinal continuity with a named regular general practitioner (RGP) and use of out-of-hours (OOH) services, acute hospital admission, and mortality. Design and setting Registry-based observational study in Norway covering 4 552 978 Norwegians listed with their RGPs. Method Duration of RGP–patient relationship was used as explanatory variable for the use of OOH services, acute hospital admission, and mortality in 2018. Several patient-related and RGP-related covariates were included in the analyses by individual linking to high-quality national registries. Duration of RGP–patient relationship was categorised as 1, 2–3, 4–5, 6–10, 11–15, or >15 years. Results are given as adjusted odds ratio (OR) with 95% confidence intervals (CI) resulting from multilevel logistic regression analyses. Results Compared with a 1-year RGP–patient relationship, the OR for use of OOH services decreased gradually from 0.87 (95% CI = 0.86 to 0.88) after 2–3 years’ duration to 0.70 (95% CI = 0.69 to 0.71) after >15 years. OR for acute hospital admission decreased gradually from 0.88 (95% CI = 0.86 to 0.90) after 2–3 years’ duration to 0.72 (95% CI = 0.70 to 0.73) after >15 years. OR for dying decreased gradually from 0.92 (95% CI = 0.86 to 0.98) after 2–3 years’ duration, to 0.75 (95% CI = 0.70 to 0.80) after an RGP–patient relationship of >15 years. Conclusion Length of RGP–patient relationship is significantly associated with lower use of OOH services, fewer acute hospital admissions, and lower mortality. The presence of a dose–response relationship between continuity and these outcomes indicates that the associations are causal. | en_US |
| dc.language.iso | eng | en_US |
| dc.publisher | Royal College of General Practitioners | en_US |
| dc.rights | Navngivelse 4.0 Internasjonal | * |
| dc.rights.uri | http://creativecommons.org/licenses/by/4.0/deed.no | * |
| dc.title | Continuity in general practice as predictor of mortality, acute hospitalisation, and use of out-of-hours care: a registry-based observational study in Norway | en_US |
| dc.type | Journal article | en_US |
| dc.type | Peer reviewed | en_US |
| dc.description.version | publishedVersion | en_US |
| dc.rights.holder | Copyright The Authors | en_US |
| cristin.ispublished | true | |
| cristin.fulltext | original | |
| cristin.qualitycode | 2 | |
| dc.identifier.doi | 10.3399/BJGP.2021.0340 | |
| dc.identifier.cristin | 1943167 | |
| dc.source.journal | British Journal of General Practice | en_US |
| dc.source.pagenumber | e84-e90 | en_US |
| dc.identifier.citation | British Journal of General Practice. 2022, 72 (715), e84-e90. | en_US |
| dc.source.volume | 72 | en_US |
| dc.source.issue | 715 | en_US |
Tilhørende fil(er)
Denne innførselen finnes i følgende samling(er)

Med mindre annet er angitt, så er denne innførselen lisensiert som Navngivelse 4.0 Internasjonal